Normal LDL-C, elevated ApoB: how often Ultrahuman's cohort carries the discordance the new guidelines target
We analysed data from more than 3,000 users and found that some people with normal LDL still had elevated ApoB levels.
LDL cholesterol measures how much cholesterol rides inside atherogenic particles. Apolipoprotein B counts the particles directly, since every LDL, IDL, VLDL, and Lp(a) particle carries exactly one ApoB on its surface. Two people with identical LDL-C can host very different particle counts, and the higher-count individual sits at materially higher cardiovascular risk. A 432,092-adult UK Biobank analysis found ApoB the stronger predictor of cardiovascular disease in men (Kelly et al., 2026). In UK Biobank participants with type 2 diabetes, ApoB reclassified the largest share of statin users whose LDL-C had already fallen to or below 100 mg/dL (Lyu et al., 2026). A March 2026 simulation argued an ApoB goal beats LDL-C and non-HDL-C targets in 65 percent of primary-prevention scenarios (Luebbe et al., 2026).
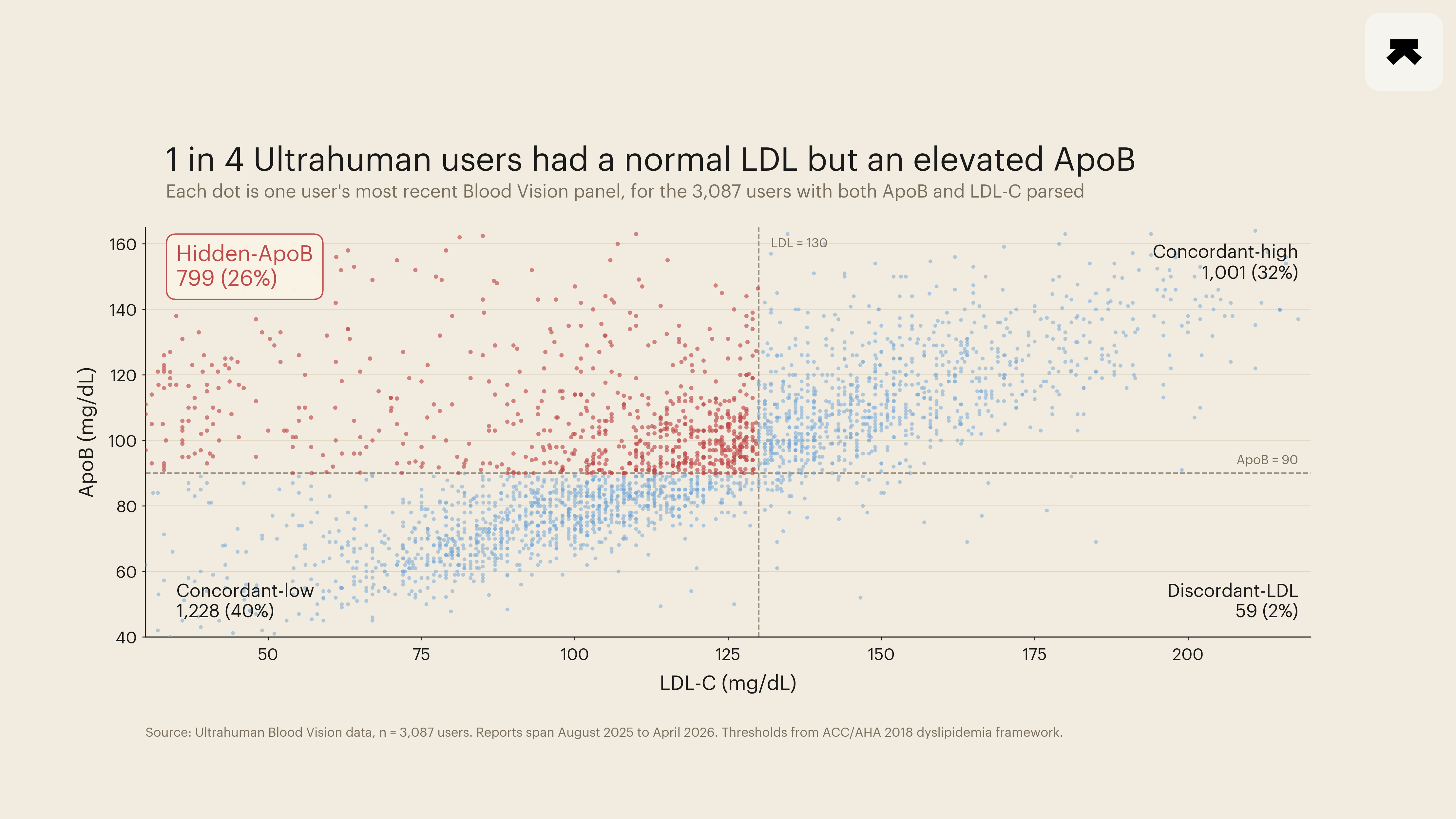
We pulled Blood Vision panels between August 2025 and April 2026 carrying both LDL-C and ApoB cleanly parsed from the lab report, giving 3,087 members. Median age 37 (IQR 31 to 44), 1,993 men and 1,038 women. Cut-points followed the ACC/AHA 2018 framework and the JAMA 2026 simulation: LDL-C below 130 mg/dL, ApoB below 90 mg/dL.
Quadrant prevalence:
- Concordant-low (LDL-C < 130, ApoB < 90): 1,228 members, 40 percent
- Concordant-high (both elevated): 1,001 members, 32 percent
- Hidden-ApoB (LDL-C < 130, ApoB ≥ 90): 799 members, 26 percent
- Discordant-LDL (LDL-C ≥ 130, ApoB < 90): 59 members, 2 percent
Of the 858 panels with discordant LDL-C and ApoB, 799 (93 percent) showed elevated ApoB with normal LDL-C; 59 (7 percent) showed the reverse.
A hidden-ApoB share near a quarter of an engaged-tracker cohort is consistent with the reasoning behind the recent guideline shift. The discordance is common enough that an LDL-only screen misses a non-trivial fraction of the people the new framing is built to catch. Among the 1,817 members with at least 10 nights of ring-recorded resting heart rate in the 30 days before their draw, the hidden-ApoB group ran a median overnight RHR of 57.0 bpm against 56.5 bpm in the concordant-low group, a 0.5 bpm gap whose bootstrap 95 percent confidence interval brushes zero. The direction matches what the literature predicts; the magnitude in cross-sectional data sits below the pre-specified 2 bpm threshold and is reported as directional only.
The 2026 guidance assumes the LDL-versus-ApoB discordance is common enough that an LDL-only screen misses meaningful risk. In 26 percent of this cohort, it did.
- Luebbe S, et al. Cost-Effectiveness of ApoB, Non-HDL-C, and LDL-C Goals for Primary Prevention Lipid-Lowering Therapy. JAMA, 2026. PMID: 41949879.
- Kelly RK, et al. Sex Differences in Lipids and Lipoproteins and Their Relationship With Cardiovascular Disease: A Prospective Study of UK Biobank Participants. Journal of the American Heart Association, 2026. PMID: 41954057.
- Lyu L, et al. Association of apolipoprotein B and excess apolipoprotein B with cardiovascular risk in type 2 diabetes: UK Biobank cohort. Lipids in Health and Disease, 2026. PMID: 41535885.