Ultrahuman Healthcare Pvt. Ltd.
Objective: Beyond the acute shock we reported earlier, populations under continued conflict exposure carry a separate chronic burden. We quantify this burden across the six weeks of the current escalation, using continuous wearable monitoring.
Methods: We analyzed 10.5 million user-nights from 197,989 Ultrahuman Ring users across 65 countries over a 72-day window (February 1 – April 13, 2026), quantifying the chronic effect across the 43-day post-escalation window (Mar 2 – Apr 13) against the Feb 1–27 baseline. Since Ramadan happened concurrently, we teased apart its impact from the war's effect in this study.
Results:
Conclusion: Chronic sleep deficits vary widely across high-exposure countries six weeks into the ongoing conflict, while weekly heart-rate rhythm cleanly separates high-exposure from reference populations. Together, these findings establish population-scale wearable monitoring as a practical tool for tracking the chronic physiological cost of geopolitical stress.
Our earlier study documented an immediate drop in population sleep score on the night of the February 28, 2026 escalation, concentrated in countries proximate to or directly affected by the conflict [1]. That analysis positioned sleep disruption as an early, objective signal of mental-health burden, amenable to population-level surveillance and preventive intervention. Here we extend that single-night snapshot into the weeks that followed to quantify the chronic effect.
As described in the previous report, broken sleep is both a symptom of acute psychological stress and a potential risk factor for later anxiety, depression, and post-traumatic stress, mediated through HPA-axis activation [2] and sympathetic nervous system arousal [3,4]. Sleep disturbance after violent or high-stress events is well documented at the clinical and small-cohort level [5,6], but population-level longitudinal physiological evidence during ongoing geopolitical events has historically been inaccessible: clinical cohorts are small and recruited post hoc, and self-report captures only what respondents can articulate. Continuous passive wearable monitoring, now deployed at population scale, addresses both constraints, with precedent in influenza-like-illness surveillance [7], pandemic detection from wearable-plus-symptom data [8], and population-scale HR/HRV characterisation [9]. The population-level mental-health burden of an active conflict is therefore well-theorised but empirically thin, particularly in the days-to-weeks window where early intervention could be most tractable.
In this study, we extend the observation to a 72-day window (February 1 – April 13, 2026) across 65 countries to quantify the chronic deficit across the weeks of ongoing conflict after February 28 and ask whether it varies across high-exposure populations. Ramadan (February 18 – March 19, 2026) overlaps most of the observation window and itself alters sleep architecture, debt, and HRV [10–13]; we factor out its contribution from the war-attributable signal as a core step of the analysis. We finally track sleep score and sleep heart rate day by day across the full observation window to trace the physiological signature of the ongoing conflict, and how that trajectory differs between high-exposure and reference populations.
We analysed 10.5 million user-nights from 197,989 Ultrahuman Ring users across 65 countries, over the 72-day observation window February 1 – April 13, 2026. The baseline window is Feb 1 – Feb 27, 2026. The acute window is February 28, 2026, the first day of sleep data reflecting the night of the escalation. The post-escalation window is Mar 2 – Apr 13, 2026 (43 days, starting the day after the acute day and including the April 8 ceasefire). Users were included if they contributed ≥7 valid nights in both the baseline and post-escalation windows; countries with fewer than 100 such users were excluded. Country labels follow location mapping, which treats administrative regions (e.g., Hong Kong, Puerto Rico) and formal state names (e.g., Russian Federation, Cyprus) as individual entries rather than rolling them up to parent jurisdictions. Per-night metrics are drawn directly from the Ring's internal algorithms: sleep score (0–100), sleep efficiency (%), total sleep duration (min), awake time (min), REM %, deep %, sleep heart rate (BPM), and stress score. Each country-day value is the mean across users active that day; post-escalation-window effects are summarized as the mean across days.
The chronic effect is the mean daily Δ from the Feb 1–27 baseline across the 43-day window (Mar 2 – Apr 13), direction-corrected, in native units. For a Ramadan-only control, we assembled a parallel 2025 cohort over Feb 1 – Apr 30, 2025 using the same eligibility criteria as 2026, with the ≥100-users-per-country threshold relaxed to ensure every country represented in the 2026 cohort would appear in the control. Ramadan 2026 ran Feb 18 – Mar 19, 2026; Ramadan 2025 ran March 1 – March 30, 2025.
For the heart-rate rhythm analysis, each country's daily sleep-HR series is compared against its own 7-day centered rolling mean (≥3 valid days per window). Weekly periodicity is quantified as the lag-7 autocorrelation of the daily series — the Pearson correlation of each day's value with the value from seven days earlier — computed over February 18 – April 8, 2026 (Ramadan start through ceasefire). A value near 1 indicates a strong weekly pattern (each day closely resembles the same weekday the prior week); a value near 0 indicates the weekly structure has broken down.
Statistical tests: Mann-Whitney U on daily Ramadan Δ values (2026 vs 2025) for each of the seven metrics; diff-in-diff t-test on pre- vs post-February-28 aggregate Δ comparing 2026 against 2025; and Mann-Whitney U on per-country lag-7 autocorrelation, high-exposure vs reference.
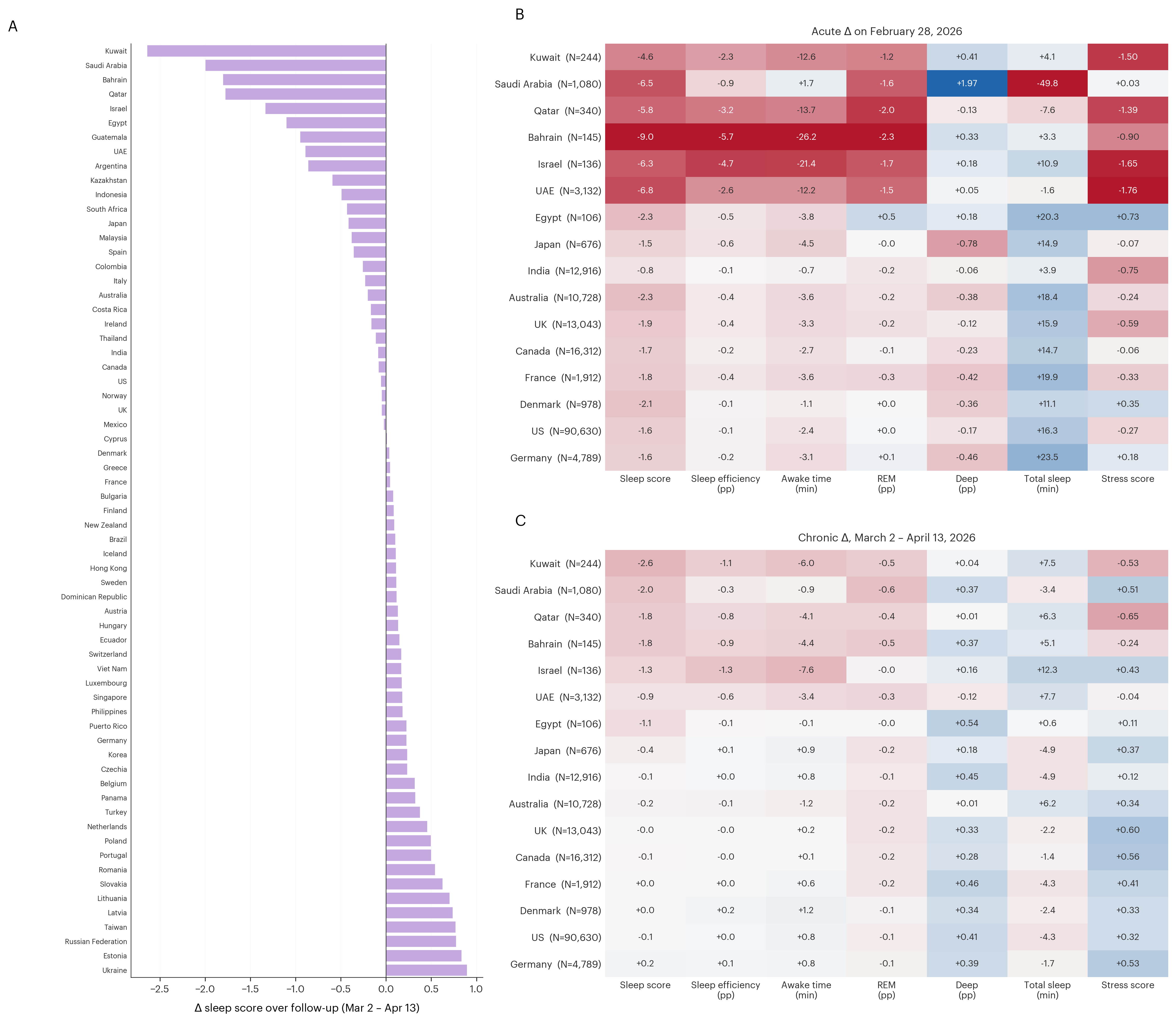
Having established the Feb 28 acute signal in the earlier report [1], we now turn to the chronic effect across the 43-day post-escalation window. Ranking all 65 cohort countries by chronic Δ sleep score (Mar 2 – Apr 13 mean minus Feb 1–27 baseline mean), the six high-exposure countries all show deficits (Figure 1A): Kuwait (−2.6 pts), Saudi Arabia (−2.0), Bahrain (−1.8), Qatar (−1.8), Israel (−1.3), and the UAE (−0.9).
The Feb 28 acute drop, recomputed on this study's 197,989-user cohort (Figure 1B), was largest in Bahrain (−9.0 pts), UAE (−6.8), Saudi Arabia (−6.5), Israel (−6.3), Qatar (−5.8), and Kuwait (−4.6). All six high-exposure countries (UAE N=3,132, SA N=1,080, Qatar N=340, Kuwait N=244, Bahrain N=145, Israel N=136) declined on every metric. Among the ten reference countries, the nine majorly non-Ramadan-observing references (Japan, India, Australia, UK, Canada, France, Denmark, US, Germany) showed small, unsystematic deviations, while Egypt (N=106), the one Ramadan-observing reference country, showed a modest sleep-score decline (−2.3 pts).
The chronic Δ sleep score (Figure 1C) was deepest in Kuwait (−2.6 pts), followed by Saudi Arabia (−2.0), Bahrain and Qatar (−1.8 each), Israel (−1.3), and the UAE (−0.9). Acute severity did not predict chronic magnitude — Bahrain's Feb 28 drop was the cohort's largest (−9.0 pts) yet its chronic deficit is moderate, while Kuwait's shallower acute drop (−4.6 pts) carries into the deepest chronic deficit. The chronic signature extends beyond sleep score. In five of six high-exposure countries, awake time rose (~3–8 min), total sleep lengthened (~5–12 min), and sleep efficiency fell (~0.6–1.3 pp) — consistent with longer but lower-quality sleep. Saudi Arabia is the exception: essentially flat awake time (−0.9 min), mildly shortened total sleep (−3.4 min), and a slight rise in sleep efficiency (−0.3 pp), despite its substantial chronic sleep-score drop. Stress score trended lower (worse) in Kuwait, Qatar, and Bahrain; Israel and Saudi Arabia trended in the opposite direction, and the UAE was near-flat. Sleep-stage composition (REM %, deep %) stayed close to baseline in all six countries.
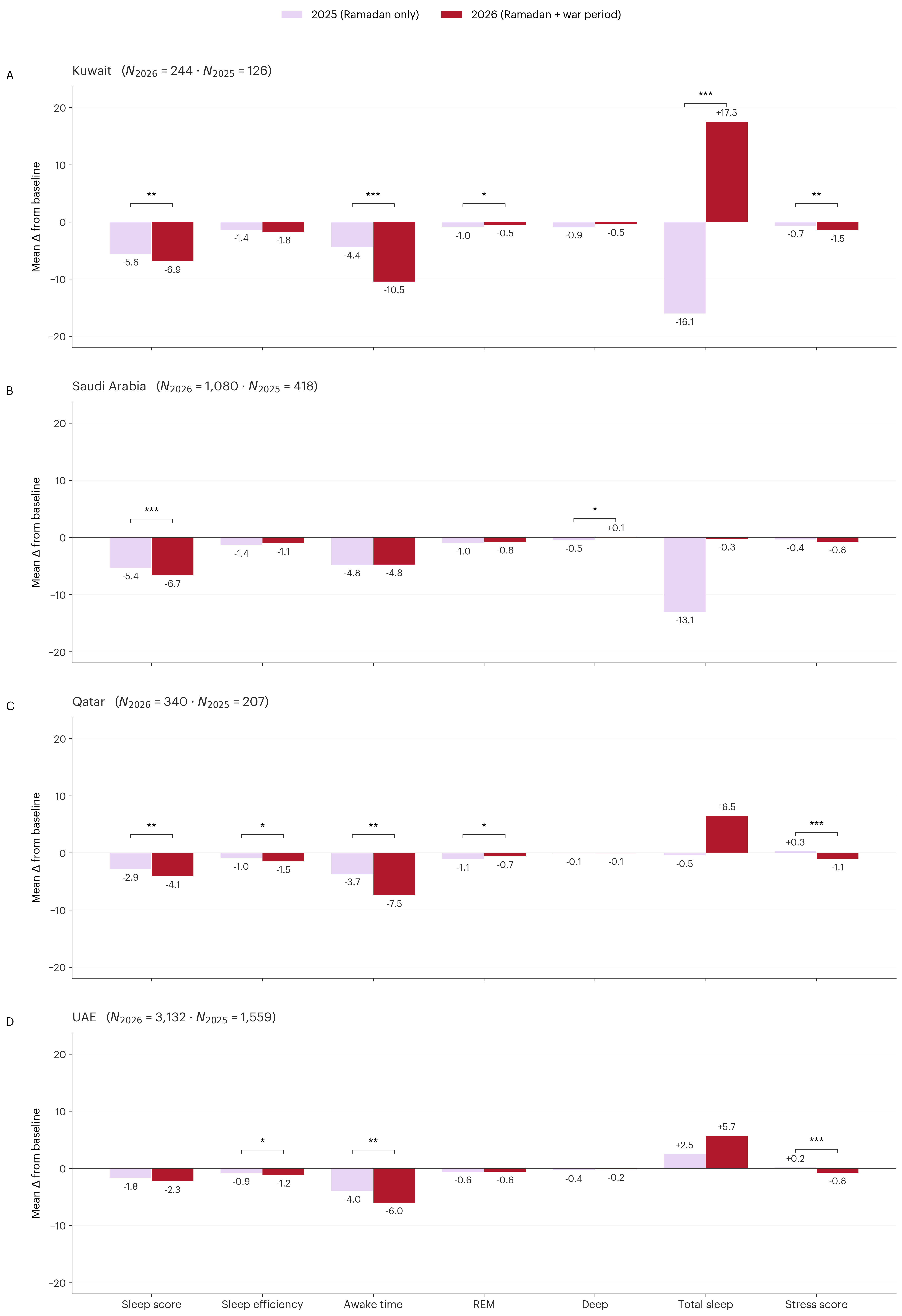
Across the four high-exposure countries with robust longitudinal samples in both years — Kuwait (N₂₀₂₆=244 · N₂₀₂₅=126), Saudi Arabia (1,080 · 418), Qatar (340 · 207), and the UAE (3,132 · 1,559) — the 30-day Ramadan 2026 sleep changes consistently exceeded those during the 2025 Ramadan period (Figure 2).
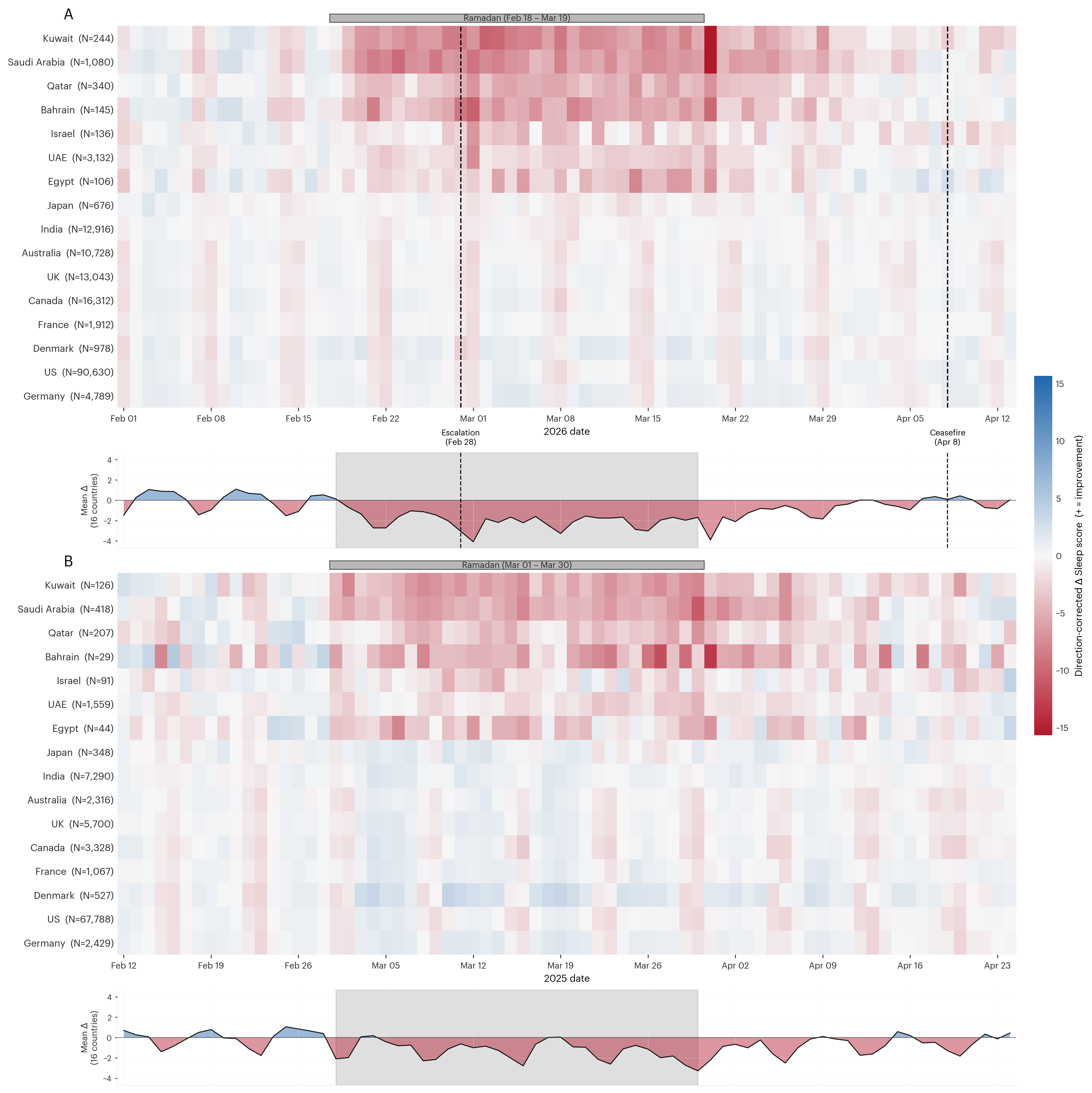
The phase-aligned 2025-vs-2026 sleep-score trajectories place the two years side by side, with each year's Ramadan start as the alignment anchor (Figure 3). The 2025 panel shows the sleep-score shift that accompanies Ramadan, visible here as a red band during and immediately after the 30-day fasting period. The 2026 panel reproduces that Ramadan-period shift and layers on a sharp additional downward inflection following the February 28 escalation. A diff-in-diff test over the 10 days before and after the escalation within each year confirms that the Feb 28 inflection is specific to 2026: the 2026 aggregate drops 0.69 pts across the Feb 28 transition, whereas 2025 moves only 0.05 pts across the matched March 11 transition (t = −1.99, p = 0.031). The 2026 red band holds through mid-April with only gradual fading, with per-country heterogeneity: Kuwait, Saudi Arabia, and Qatar remain visibly red through April 13, while Bahrain, Israel, and the UAE fade earlier.
Reference-country rows show a regular weekly rhythm of weekend sleep-score drops, preserved across both years. In the Ramadan-observing and war-exposed countries that same rhythm is essentially masked at the heatmap level, where the Ramadan red band and, in 2026, the Feb 28 war effect dominate, but it re-emerges in the 16-country aggregate curve beneath each heatmap: cleanly preserved in 2025 and visibly shifted in 2026 from the Feb 28 transition onward (Figure 3).
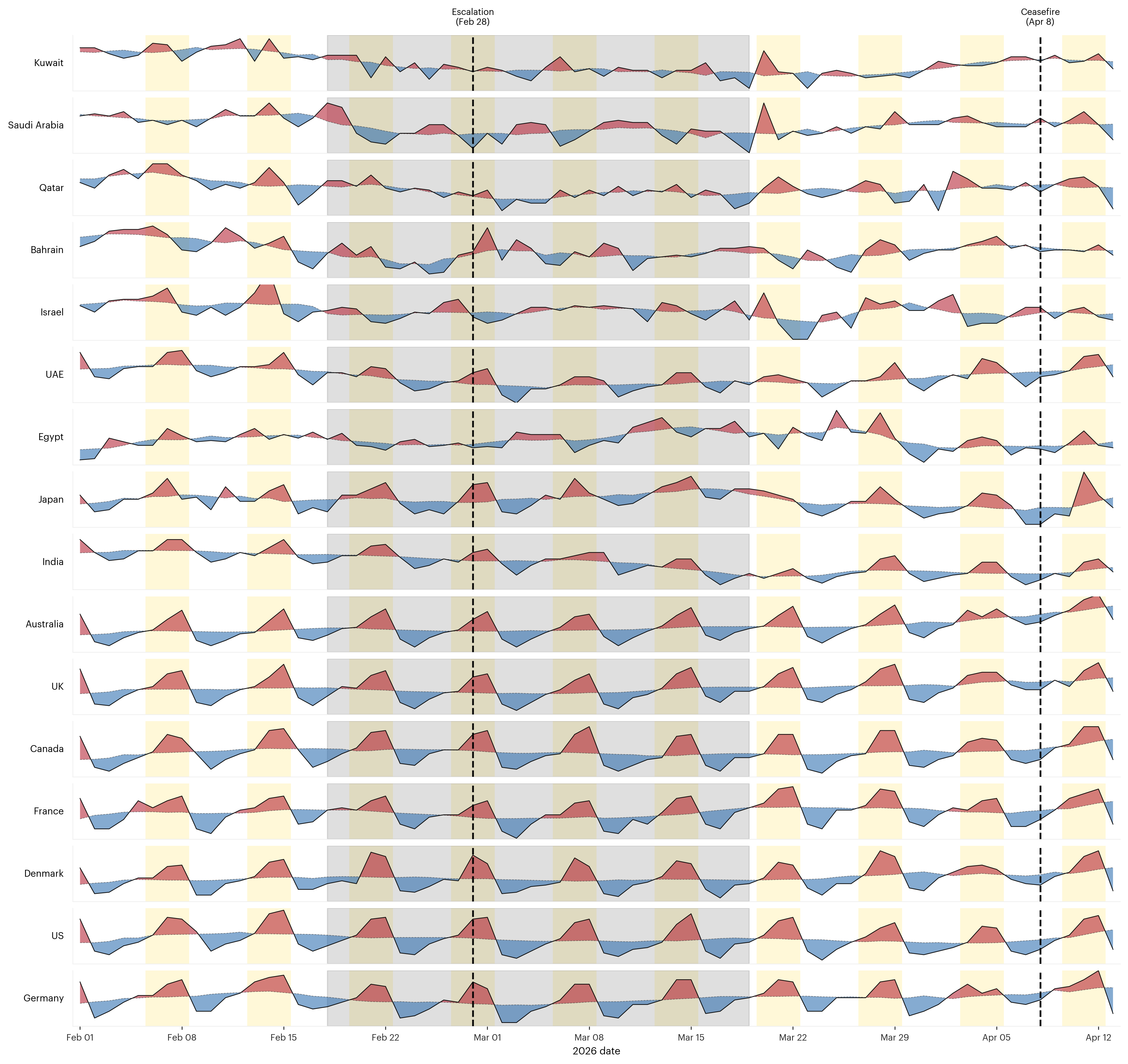
The weekly heart-rate rhythm panel (Figure 4) tracks a second view of the same population across three recognizable phases. In the pre-escalation window (Feb 1–17), every country shows a visible weekly HR oscillation aligned to its local workweek cadence; weekend conventions vary (Fri–Sat in Bahrain, Kuwait, Qatar, Saudi Arabia, Egypt, and Israel; Sat–Sun elsewhere), so the rhythm's phase differs by country, but a rhythm is present in each. From the Ramadan start on February 18, this weekly rhythm is disrupted in the Ramadan-observing countries while the non-Ramadan-observing reference countries rhythm continues unperturbed. After Ramadan ends on March 19, Egypt, the UAE, and the majorly non-Ramadan reference countries re-establish their weekly rhythm, whereas Kuwait, Saudi Arabia, Qatar, Bahrain, and Israel remain largely flat through the April 8 ceasefire and into mid-April. Quantitatively, the lag-7 autocorrelation of each country's daily sleep-HR series over Feb 18 – Apr 8, 2026 is 0.12 for the six high-exposure countries (range −0.18 to +0.66) versus 0.81 for the ten reference countries (range +0.21 to +0.97); the difference is highly significant (Mann-Whitney U, one-sided; p < 0.001).
Both the sleep-score trajectory (Figure 3) and the weekly heart-rate rhythm (Figure 4) separate high-exposure countries from reference countries across the war period.
Building on our prior report of the acute February 28 response [1], continuous day-by-day passive physiological tracking across the 43-day post-escalation window establishes the chronic effect at population scale. The mental-health burden of an active conflict is well-theorised from clinical and small-cohort work [5,6] but empirically thin at population scale, especially in the days-to-weeks window where early intervention could be most tractable. Across the 43-day post-escalation window, the response to the February 28 escalation is sharply heterogeneous across high-exposure countries: Kuwait, Saudi Arabia, and Qatar show the deepest chronic sleep-score Δ (−2.6, −2.0, −1.8 pts; Fig. 1C), while Bahrain, Israel, and the UAE show smaller chronic deficits (−1.8, −1.3, −0.9). The same country-level pattern holds on both axes: the UAE, with the smallest chronic sleep deficit among the high-exposure set, is also the one country that re-established its weekly HR rhythm (lag-7 autocorrelation = +0.66), while the remaining five high-exposure countries combine chronic sleep deficits with flattened rhythms (lag-7 range −0.18 to +0.25). Acute severity did not predict chronic magnitude. For instance, Bahrain's Feb 28 drop was the cohort's largest (−9.0 pts) yet its chronic deficit is moderate, while Kuwait's shallower acute drop (−4.6 pts) carries into the deepest chronic deficit. These patterns point to on-the-ground factors such as persistent threat, displacement, and infrastructure disruption that physiology registers but does not directly name. This war-attributable signal was separated from the overlapping Ramadan effect on sleep and HRV [10–13] via a matched 2025 Ramadan-only cohort; the 2026 increment above that baseline is what we assign to the conflict.
Looking at which metrics moved and which did not, we read a specific physiological pattern. The war-attributable increment concentrates on sleep quantity (time in bed, awake time, total sleep) and on the stress score, while sleep-stage architecture (REM %, deep %) stays largely intact. We interpret this as a pattern of extended sleep time with degraded quality, consistent with chronic HPA-axis activation under sustained psychological stress [2] and with the persistent emotional-regulation demand described in the sleep–affect literature [16]: populations that sleep longer but worse, and register higher stress scores at night. We read the weekly-rhythm flattening, in chronobiological terms, as the disappearance of the weekday-versus-weekend social-jetlag contrast [17,18] — either because the daily routine that produces it is itself disrupted or because biological responses to retained structure are suppressed, or both.
Beyond the specific findings, our results position daily sleep score and weekly heart-rate rhythm as practical, passive biomarkers of population-scale physiological and mental-health burden. These signals are sensitive enough to register an acute geopolitical shock and specific enough to separate a war-attributable increment from overlapping Ramadan effects, and (for HR rhythm) structured enough to index whether normal weekly routine has returned. Because the rhythm resets as weekly structure returns, it offers a natural short- and long-term recovery marker that can be tracked week by week as a conflict de-escalates, or compared across populations emerging from different kinds of collective stress. Our study thus does more than quantify the chronic response: it lays out a passive, population-scale monitoring framework for assessing the mental-health burden of active conflict via day-by-day physiological observation.
1. Shet, A., Agarwal, A., Gupta, K., Dhawale, N., Narasimhan, V.,& Srinivasan, B. (2026). Population-Scale Ring AIR Monitoring CapturesGeographic Patterns of Acute Sleep Disruption Amidst Geopolitical Conflict. https://science.ultrahuman.com/studies/impact-of-conflict-on-sleep-and-mental-health
2. Buckley, T. M., & Schatzberg, A. F. (2005). On theinteractions of the hypothalamic-pituitary-adrenal (HPA) axis and sleep: normalHPA axis activity and circadian rhythm, exemplary sleep disorders. Journal ofClinical Endocrinology & Metabolism, 90(5), 3106–3114.
3. Thayer, J. F., Åhs, F., Fredrikson, M., Sollers, J. J., &Wager, T. D. (2012). A meta-analysis of heart rate variability and neuroimagingstudies: implications for heart rate variability as a marker of stress andhealth. Neuroscience & Biobehavioral Reviews, 36(2), 747–756.
4. Kim, H.-G., Cheon, E.-J., Bai, D.-S., Lee, Y. H., & Koo,B.-H. (2018). Stress and heart rate variability: A meta-analysis and review ofthe literature. Psychiatry Investigation, 15(3), 235–245.
5. Palmieri, P. A., Chipman, K. J., Canetti, D., Johnson, R. J.,& Hobfoll, S. E. (2010). Prevalence and correlates of sleep problems inadult Israeli Jews exposed to actual or threatened terrorist or rocket attacks.Journal of Clinical Sleep Medicine, 6(6), 557–564.
6. Germain, A. (2013). Sleep disturbances as the hallmark of PTSD:where are we now? American Journal of Psychiatry, 170(4), 372–382.
7. Radin, J. M., Wineinger, N. E., Topol, E. J., & Steinhubl, S.R. (2020). Harnessing wearable device data to improve state-level real-timesurveillance of influenza-like illness in the USA: a population-based study. TheLancet Digital Health, 2(2), e85–e93.
8. Quer, G., Radin, J. M., Gadaleta, M., Baca-Motes, K., Ariniello,L., Ramos, E., Kheterpal, V., Topol, E. J., & Steinhubl, S. R. (2021).Wearable sensor data and self-reported symptoms for COVID-19 detection. NatureMedicine, 27(1), 73–77.
9. Natarajan, A., Pantelopoulos, A., Emir-Farinas, H., &Natarajan, P. (2020). Heart rate variability with photoplethysmography in 8million individuals: a cross-sectional study. The Lancet Digital Health, 2(12),e650–e657.
10. Roky, R., Houti, I., Moussamih, S., Qotbi, S., & Aadil, N.(2004). Physiological and chronobiological changes during Ramadan intermittentfasting. Annals of Nutrition and Metabolism, 48(4), 296–303.
11. BaHammam, A. S. (2006). Does Ramadan fasting affect sleep? InternationalJournal of Clinical Practice, 60(12), 1631–1637.
12. Qasrawi, S. O., Pandi-Perumal, S. R., & BaHammam, A. S.(2017). The effect of intermittent fasting during Ramadan on sleep, sleepiness,cognitive function, and circadian rhythm. Sleep and Breathing, 21(3), 577–586.
13. Krishnan, N., Asudani, V., Singh, P., Singhal, V., Srinivasan,B., & Bhattacharya, A. (2024). Chronic sleep debt manifests over time,independent of coping strategies, during Ramadan fasting: an exploratory studyusing the Ultrahuman Ring AIR. https://science.ultrahuman.com/studies/ramadan-sleep-debt
14. Asudani, V., Krishnan, N., Singh, P., Singhal, V., Srinivasan,B., & Bhattacharya, A. (2024). Modifying sleep tracking algorithms revealsspecific sleep deprivation patterns in women: early findings from theUltrahuman Ring AIR Ramadan Mode. https://science.ultrahuman.com/studies/ramadan-mode-sleep-debt-in-women
15. Asudani, V., Krishnan, N., Singh, P., Singhal, V., Srinivasan,B., & Bhattacharya, A. (2024). Impact of age and BMI on sleep metrics inindividuals with chronic sleep deprivation: Pooled analyses from the UltrahumanRing AIR Ramadan study. https://science.ultrahuman.com/studies/coping-with-chronic-sleep-debt-do-age-and-bmi-matter
16. Goldstein, A. N., & Walker, M. P. (2014). The role of sleepin emotional brain function. Annual Review of Clinical Psychology, 10, 679–708.
17. Wittmann, M., Dinich, J., Merrow, M., & Roenneberg, T.(2006). Social jetlag: misalignment of biological and social time. ChronobiologyInternational, 23(1-2), 497–509.
18. Roenneberg, T., Allebrandt, K. V., Merrow, M., & Vetter, C. (2012). Social jetlag and obesity. Current Biology, 22(10), 939–943.