Resting heart rate percentile bands by age and sex in 229,963 ring wearers, with the within-peer-group RHR ladder rendered nightly
We report a age- and sex-matched normative reference for overnight resting heart rate that members can match their data to.
Resting heart rate carries one of the cleanest population-mortality signals in cardiology, and the signal has held up across decades of prospective epidemiology and one of the largest dose-response meta-analyses in the field. A 16-year follow-up of 2,798 men in the Copenhagen Male Study, originally measured by resting ECG, established that every 10 bpm higher RHR carried a 16 percent higher all-cause mortality risk (95 percent CI 10 to 22 percent), with the effect surviving adjustment for cardiorespiratory fitness, leisure activity, smoking, and other standard cardiovascular risk factors (Jensen et al., 2013). The most comprehensive modern synthesis is a dose-response meta-analysis of 87 prospective cohort studies that placed the per-10-bpm relative risk at 1.15 for cardiovascular disease, 1.14 for total cancer and 1.17 for all-cause mortality, with a linear dose-response from approximately 60 bpm upward (Aune et al., 2017). What both lines of evidence leave unresolved is the within-individual translation: at the level of a single user's nightly autonomic state, what does the 10-bpm-per-10-bpm mortality ladder look like?
The 229,963-member Ultrahuman ring cohort offers two complementary reads. First, normative percentile bands of overnight resting heart rate by decade and sex, which let an individual locate where their reading sits within their peer group. Second, the within-peer-group ladder: among members in the same decade and sex cell, the highest-RHR fifth runs 17 to 28 ms lower in overnight HRV and 5 to 9 points lower on the ring's composite Dynamic Recovery score than the lowest-RHR fifth, with the direction holding identically in every one of ten cells.
Cohort definition. Eligible members were external Ultrahuman ring users with at least 21 valid overnight RHR nights in the 90-day window from 24 January to 24 April 2026, where validity required a valid sleep score and a non-null resting heart rate value within a plausibility window of 30 to 120 bpm. Internal users were excluded at the SQL level, age was constrained to 18 to 90 with binary gender recorded, and per-user inclusion required the 21-night threshold. The resulting cohort split into 10 decade-by-sex cells, the smallest of which (60+ female) carried 5,033 members; the largest (18-29 female) carried 80,445. Cell sizes reflect the known female skew of the young-adult Ultrahuman ring base. Per-user metrics were the within-window median of RHR; cell-level descriptive statistics included sample percentiles P10, P25, P50, P75 and P90 of those per-user medians. The secondary analysis split each cell into RHR quintiles (Q1 = lowest, Q5 = highest) and reported the cell-by-quintile means of overnight HRV, Dynamic Recovery score and sleep efficiency. Smallest quintile sub-cell carried 1,006 members.
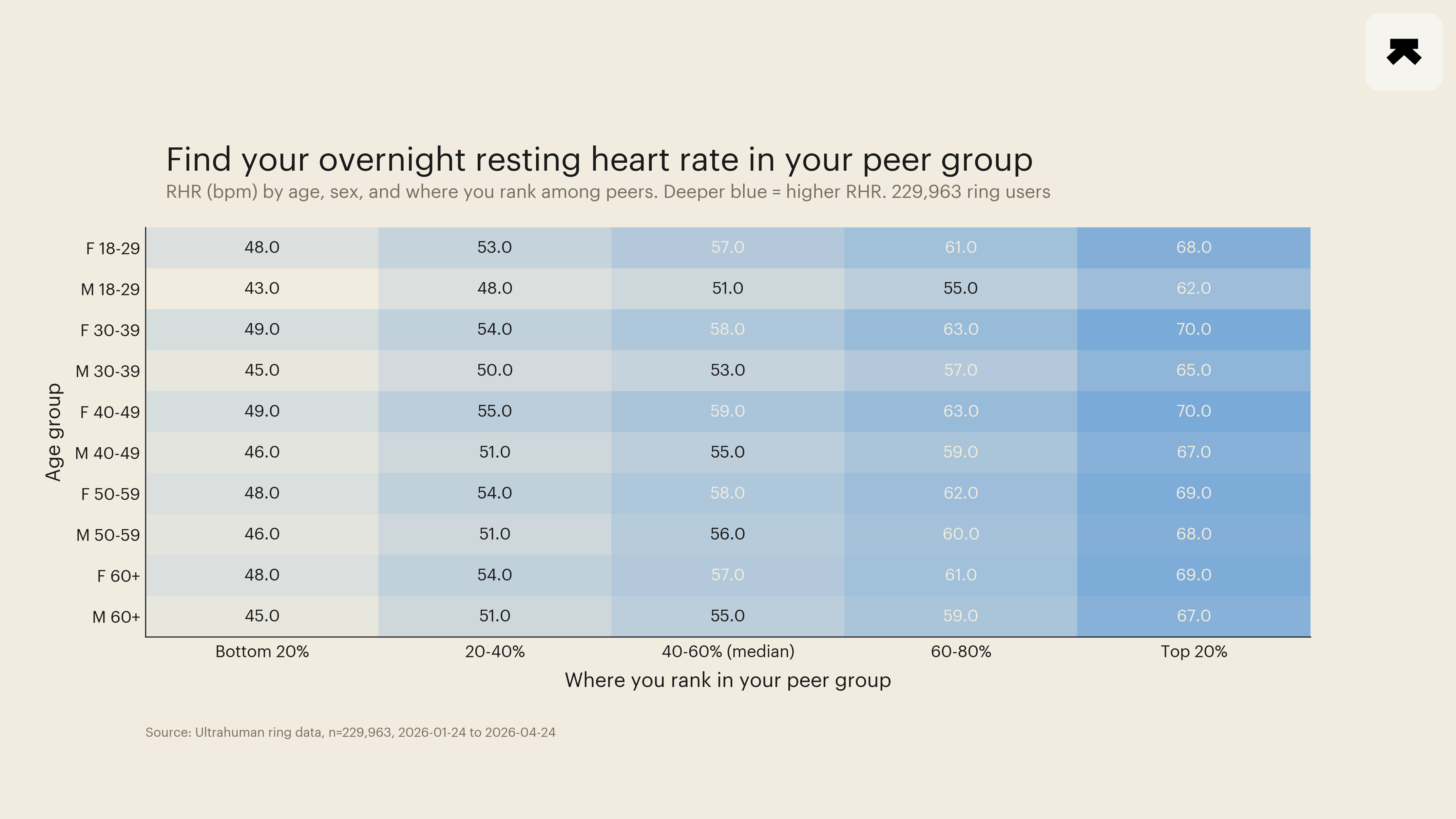
Two structural features of the percentile bands are worth naming. The first is a 5-to-6-bpm sex gap that holds at every decade, with women's median RHR running consistently above men's. In the 18-29 band, female P50 sat at 57 bpm and male P50 at 51 bpm; the same gap held in every other decade (30-39: 58 vs 53; 40-49: 59 vs 55; 50-59: 58 vs 55.5; 60+: 57 vs 55). The gap is well-established physiology and reflects smaller chamber size and lower stroke volume in women, requiring a higher heart rate to maintain the same cardiac output. It is not a health difference. The second is the modest decade drift: median RHR rises approximately 2 bpm from the 18-29 band to the 40-49 band and then plateaus or modestly declines. Read against the general-population pattern in which RHR slowly rises across the adult lifespan, the plateau-after-40 shape in this cohort is consistent with a healthy-wearer selection effect: the long-term-tracker cohort over 40 is healthier than the general-population baseline at the same age. The plateau is a cohort artefact of self-selection, not a physiological stop in the underlying age trend.
The percentile bands themselves are the actionable read. P10-to-P90 spans approximately 19 to 20 bpm in every cell. P25-to-P75 spans approximately 10 bpm. Two perfectly healthy 30-year-old women in the cohort can carry overnight resting heart rates of 49 and 69 bpm and both sit within the central 80 percent of their peer group. The implication is that "is my number average for my age" is a less informative question than "where am I in my band." A normative cell-by-cell percentile chart is the right object to read against, not a single population mean.
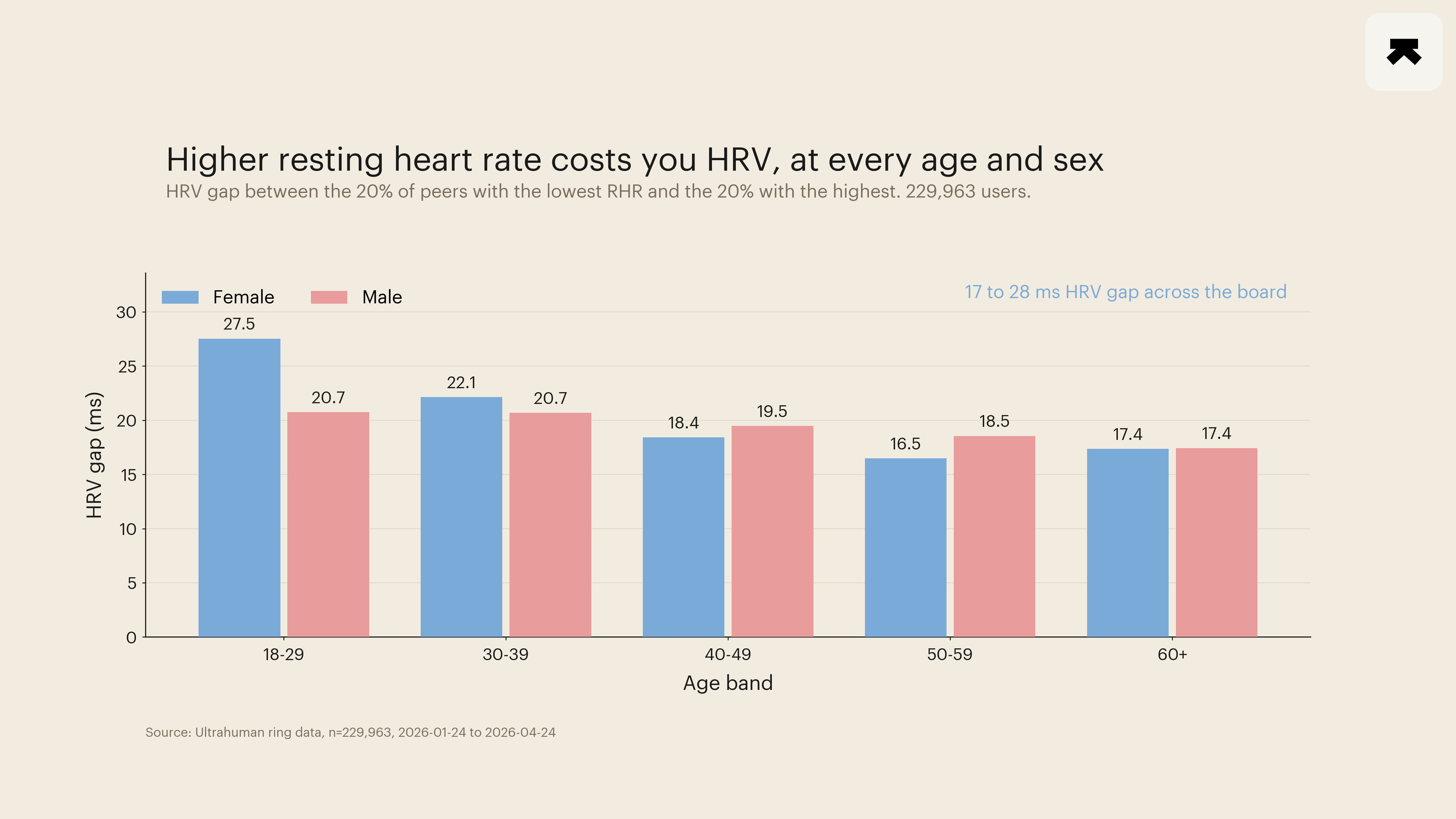
The within-peer-group ladder. Within each of the ten decade-by-sex cells, the per-user median RHR was binned into five quintiles. Q5-minus-Q1 RHR gaps ran approximately 20 bpm across every cell (47.6 to 67.7 bpm in 18-29 women; 43.0 to 61.6 bpm in 18-29 men; comparable gaps in older cells). Q5-minus-Q1 HRV deltas ran -27.5 ms (18-29 F), -20.7 ms (18-29 M), -22.1 ms (30-39 F), -20.7 ms (30-39 M), -18.4 ms (40-49 F), -19.5 ms (40-49 M), -16.5 ms (50-59 F), -18.6 ms (50-59 M), -17.4 ms (60+ F), -17.4 ms (60+ M). Q5-minus-Q1 Dynamic Recovery score deltas ran -5.1 to -8.5 points across the same cells. Sleep efficiency dropped 1 to 2 percentage points across the same axis. Cohen's d on every Q5-versus-Q1 within-cell HRV contrast exceeded 1.5 with at least 1,000 members per quintile, placing the 95 percent CIs on the differences within tighter than ±0.5 ms. The direction of the ladder is identical in every cell: members in the highest-RHR fifth of their own peer group carry materially worse autonomic and recovery markers than members in the lowest-RHR fifth.
Scaling to the literature's yardstick. Translating the Q5-versus-Q1 contrasts to a per-10-bpm-of-RHR rate gives an HRV cost of approximately 8 to 14 ms per 10 bpm and a recovery-score cost of approximately 3 to 4 points per 10 bpm, both estimated within peer groups (so age and sex are held constant). The Jensen and Aune mortality estimates per 10 bpm of RHR run 16 percent and 17 percent higher all-cause mortality respectively. The wearable-cohort numbers and the population-mortality numbers are not directly comparable in units, but the gradient is the same in direction and the within-cell magnitude of the autonomic-and-recovery cost is large by the standards of overnight wearable signal. The biology that drives the population-mortality finding is operating at the level of nightly cardiovascular and autonomic state in a way the ring is sensitive to.
Two methodological notes. The ring's overnight resting heart rate is taken during sleep and is systematically lower than a clinical seated resting heart rate measured in a physician's office, typically by 5 to 10 bpm. The percentile bands here are therefore not directly comparable to clinical norms; they are a within-instrument, within-cohort normative chart. Aerobic fitness, the strongest known correlate of resting heart rate at the individual level (Kodama et al., 2009 reported approximately 13 percent lower all-cause mortality per 1-MET higher cardiorespiratory fitness across 33 studies and 102,980 participants), is not measured in this analysis; the within-peer-group ladder reported here cannot distinguish how much of the Q5-versus-Q1 RHR gap reflects fitness versus other contributors (medication, sleep-disordered breathing, anaemia, thyroid dysfunction, chronic illness). The Jensen 2013 paper specifically demonstrated that the RHR mortality signal survives adjustment for cardiorespiratory fitness, which suggests that fitness alone does not account for the full cross-sectional ladder; the present analysis is consistent with that finding but does not independently establish it.
Caveats worth naming. The cohort is observational, the framing is associational, and the analysis does not establish that lowering an individual's resting heart rate would shift their HRV or Dynamic Recovery score by the within-cell magnitudes reported here. Reverse causation cannot be excluded: members with subclinical illness can carry higher RHR and worse HRV without one being causally upstream of the other. Selection effects are present in the standard direction for an active-tracking cohort: the percentile bands describe the Ultrahuman wearer base and not the general population. Q5-versus-Q1 within-cell estimates may be sensitive to the choice of quintile boundary; sensitivity to that choice has not been reported here. The mortality estimates from Jensen and Aune are decade-scale population predictions and do not translate to individual risk forecasts at the resolution of a single user's overnight reading.
What this analysis adds is a cohort-resolved normative reference for overnight resting heart rate at the resolution of decade and sex, in a sample two orders of magnitude larger than the largest individual prospective study cited above, paired with a within-peer-group ladder that renders the same RHR gradient that drives population mortality as a measurable nightly autonomic and recovery cost. The right way to read an individual ring reading is against the percentile bands of the corresponding peer group; the right way to track change over time is against the trend within that band, not against a single population mean.
- Jensen MT, Suadicani P, Hein HO, Gyntelberg F. Elevated resting heart rate, physical fitness and all-cause mortality: a 16-year follow-up in the Copenhagen Male Study. Heart, 2013. PMID: 23595657.
- Aune D, Sen A, o'Hartaigh B, Janszky I, Romundstad PR, Tonstad S, Vatten LJ. Resting heart rate and the risk of cardiovascular disease, total cancer, and all-cause mortality: a systematic review and dose-response meta-analysis of prospective studies. Nutrition, Metabolism and Cardiovascular Diseases, 2017. PMID: 28552551.
- Kodama S, et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA, 2009. PMID: 19454641.