Bedtime regularity, not duration, tracks overnight resting heart rate in 103,490 ring wearers
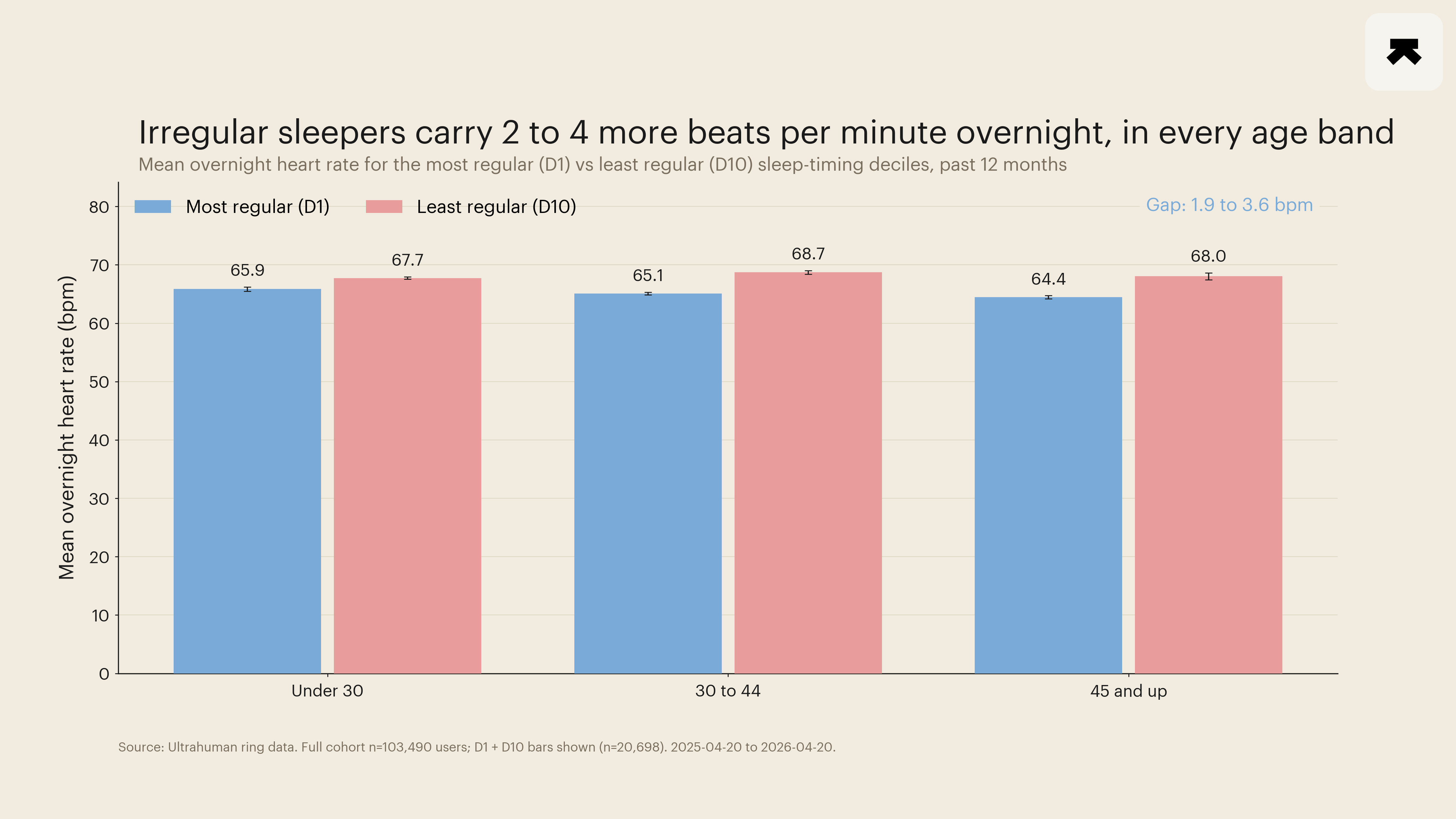
The most irregular sleepers run 1.9 to 3.6 beats per minute higher overnight than the most regular ones, in every age band, matching what large sleep studies predicted.
The hypothesis that timing regularity, rather than total time in bed, is the load-bearing sleep variable for cardiovascular health has been gathering weight in the literature since 2017, when a Boston team formalised the Sleep Regularity Index (SRI) as a 24-hour-lagged state-match probability scaled from 0 to 100 (Phillips et al., 2017). The shift accelerated in 2024 with a 60,977-participant UK Biobank actigraphy analysis showing that SRI quintiles outperformed total sleep time as a predictor of all-cause, cancer, and cardiometabolic mortality over a median 7.8 years of follow-up, with hazard ratios for the most-regular versus least-regular quintile clustering in the 0.52 to 0.80 range across cause groupings (Windred et al., 2024). A 2025 follow-up in 82,391 UK Biobank participants then extended the signal to incident dementia, with members carrying an SRI of 70 or above showing a 26 percent lower hazard than those below (Bian et al., 2025). The open question those papers leave is whether the same regularity gradient that maps onto multi-year mortality risk shows up on a consumer ring at the level of a single short-window autonomic readout. Across 103,490 long-term Ultrahuman ring wearers, it does.
The least-regular sleep-timing decile within each age band ran 1.9 to 3.6 bpm higher in mean overnight resting heart rate than the most-regular decile, with every cell's 95 percent confidence interval excluding zero.
Phillips and colleagues defined SRI on a 1-minute binary asleep-versus-awake state grid, which a ring's nightly bed-start and wake-end timestamps do not directly produce. We therefore used the standard midpoint-dispersion proxy, taking the per-user standard deviation of sleep midpoint time-of-day across qualifying nights, with a wrap-around anchor so midpoints that straddle midnight remain comparable. This proxy captures the same construct Phillips and colleagues scored, namely night-to-night timing jitter, and is closely correlated with the full state-match probability without being identical to it. Where the distinction matters, we name it; we do not call this metric SRI itself.
Cohort inclusion was deliberately tight to focus on long-term active wearers. Eligible members had at least 180 valid sleep nights in the 12 months ending 20 April 2026 and at least 30 of those nights in the most recent 90 days, with each retained night requiring a recorded total sleep of at least 180 minutes. The resulting cohort of 103,490 members carried a mean of 263 valid nights over the year and splits cleanly into ten regularity deciles within each of three age bands (under 30, 30 to 44, 45 and up). The smallest single decile-by-age cell carried 938 members.
The primary readout was mean overnight resting heart rate per decile-by-age cell, with 95 percent normal-approximation confidence intervals on the cell mean and on the decile-1-versus-decile-10 difference. In the under-30 band, decile 1 ran 65.86 bpm and decile 10 ran 67.74 bpm, a 1.88 bpm gap (95 percent CI 1.47 to 2.29). In the 30-to-44 band, the corresponding values were 65.09 and 68.72 bpm, a 3.63 bpm gap (CI 3.25 to 4.00). In the 45-and-up band, 64.44 and 68.04 bpm, a 3.60 bpm gap (CI 2.95 to 4.24). The pattern was monotonic across deciles in all three bands, not just at the endpoints. We did not fit a regression to control for sleep duration. We instead ran the same decile-1-versus-decile-10 contrast within each age band's median split on total sleep time, and the gap persisted in both the shorter-sleeping and longer-sleeping halves. Mean overnight HRV moved in the expected opposite direction, falling 1.43, 1.82, and 1.83 ms from decile 1 to decile 10 across the three age bands. Two autonomic recovery markers moving together is not a coincidence on this cohort size (Figure 1).
The pooled, age-unstratified view of the same cohort is flat. That looks like a null until the age structure of the deciles is examined. Less-regular sleepers in this cohort skew younger and therefore carry lower baseline resting heart rates and higher baseline HRV; pooling across ages buries the within-age effect under the between-age effect. Stratifying clarifies it. The pooled-versus-stratified discrepancy is a textbook Simpson's-paradox configuration, and reporting only the pooled view would have understated the underlying signal.
A 3-bpm overnight resting heart rate gap is, on its own, modest. It is the kind of difference that separates sedentary from moderately active middle-aged adults in epidemiological cohorts, and it is large enough to be measurable on commodity-grade nocturnal pulse data without overlapping confidence intervals at this n.
What gives the finding its weight is that it lines up with the direction and magnitude that the Windred and Bian papers would predict from population-mortality and population-dementia data, on a wholly different design (within-person ring readouts rather than multi-year follow-up of a national cohort) and on a different operationalisation of regularity (midpoint standard deviation rather than the full Phillips and Klerman state-match probability). Concordance across designs and metrics is what makes a population-scale wearable signal credible.
Three caveats sit on this read. The cohort is self-selected for ring use, and members with at least 180 qualifying nights in a year are by construction long-term wearers, not a general-population sample; the irregular-sleeper deciles in this cohort therefore sit on a lower-irregularity floor than a general population would. The midpoint-SD proxy is closely related to but not identical to the full Phillips and Klerman SRI. And the design is observational, with no causal claim being made about the effect of bedtime intervention on overnight heart rate; shift work, caregiving load, and chronic illness are all plausible upstream drivers that the ring cannot see.
What it does say is narrow and falsifiable. In a long-term ring cohort large enough to wash out age structure within strata, the timing-regularity gradient predicted by the literature shows up at the level of mean overnight resting heart rate, in every age band, with effect sizes consistent with the gradient seen in the population-mortality literature and exceeding 5 percent relative difference in the 30-and-up bands. Bedtime regularity is doing measurable work on overnight cardiovascular markers, on top of and not because of how long members are sleeping.
- Phillips AJK, Klerman EB, Czeisler CA, et al. Irregular sleep/wake patterns are associated with poorer academic performance and delayed circadian and sleep/wake timing. Scientific Reports, 2017. PMID: 28607474.
- Windred DP, Burns AC, Lane JM, et al. Sleep regularity is a stronger predictor of mortality risk than sleep duration: a prospective cohort study. Sleep, 2024. PMID: 37738616.
- Bian Z, et al. Association of sleep regularity index with incident dementia and brain structural changes: a prospective cohort study. BMC Public Health, 2025. PMID: 39920677.